Statins are a class of drug that, in theory, work by lowering LDL (low-denstity lipoprotein) levels. They do this by inhibiting HMG-CoA reductase, an enzyme that has a central role in the production of cholesterol in the liver. LDL, the so-called 'bad' cholesterol, isn't actually just cholesterol, but has been linked to risk of heart disease because, as a lipoprotein, its job is to transport cholesterol to and from cells. It is bound to cholesterol. What's measured when we have our blood drawn for a cholesterol test is LDL-C, the amount of cholesterol bound to LDL particles (LDL-C), as well as HDL-C, the 'good' cholesterol package, which transports LDL-C from cells, leading to lower blood cholesterol levels. Cholesterol makes plaque and plaque lines and hardens arteries, which occludes them and leads to stroke and heart attack. Lower the amount of LDL, and you lower the risk of arterial plaque deposits.
The connection between cholesterol and heart disease was first identified in the Framingham Study in the 1950's and 60's, and this lead directly to the search for drugs to lower cholesterol. Statins were developed in the 1970's and 80's, and after some fits and starts, began to be used in earnest in the late 1980's. Statins work by inhibiting the liver cells' synthesizing of new cholesterol, that is, cholesterol that isn't due taken in in the diet.
Akira Endo, one of the first scientists to look for cholesterol-lowering compounds, reviewed the history of statins in 2010. He described the many studies of the effects of these drugs, saying "The results in all these studies have been consistent: treatment with statins lowers plasma LDL levels by 25–35% and reduces the frequency of heart attacks by 25–30%" (Akira Endo, Proc Japan Acad, Series B, 2010).
A systematic review of the literature on the effectiveness of statins was published by the Cochrane Organization in 2012. The review reports, "Of 1000 people treated with a statin for five years, 18 would avoid a major CVD event which compares well with other treatments used for preventing cardiovascular disease." This suggests, of course, that 982 people took statins with no benefit, and perhaps some risk, as statins are associated with muscle pain, slightly increased risk of type 2 diabetes, liver damage, neurological effects, digestive problems, rash and flushing, and other effects. But more on this below.
So, who should take statins?
Until 2013, the recommendation was that anyone with a modest risk, as assessed by the Framingham Risk Calculator (I've read that that means from 6.5% to 10% 10-year risk) would likely be prescribed statins. The interesting thing, to me, about this risk calculator is that it's impossible to push the risk estimate past "greater than 30%", even at maximum allowable cholesterol, LDL, and systolic blood pressure, and being a smoker on blood pressure medication. Which means that there's a lot that this calculator can't tell us about our risk of CVD, based on the best risk factors known.
 |
| Framingham Risk Calculator |
In 2013, the American Heart Association/American College of Cardiology revised their criteria for statins. Now, they are recommended for people who have had one CVD event in order to prevent another; for people with primary elevations of LDL-C greater than 190mg/dL; people 45-70 years old who have diabetes and LDL-C between 70 and 189mg/dL, and people 45-70 years old with LDL-C between 70 and 189mg/dL and estimated 10-year cardiovascular disease risk of 7.5% or higher.
The first three criteria are straightforward. If statins lower LDL, and lower LDL lowers risk of ASCVD (artherosclerotic cardiovascular disease), then taking them should be beneficial. But then we're back to a risk calculator again to estimate 10-year risk.
 |
| ACC/AHA |
It has been revised. Now included are ethnicity (well, White, African American or other), and diabetic status (yes/no), and estimated lifetime risk. And, now it's possible to push 10-year risk up past 70%, which I discovered by playing around with the calculator a bit. Whether or not it's a more accurate predictor of a cardiovascular event is another question.
Here's the lowest risk I could come up with, 0.1% 10-year risk. The recommendations offered are not to prescribe statins.
 |
| Lowest 10-year risk |

Compared with the Framingham calculator, risk estimation seems to be getting more precise. Or at least bolder, with estimates up in the 70's. But is the new calculator actually better at predicting risk than the old one? A paper was recently published in JAMA addressing just this question ("Guideline-
Based Statin Eligibility, Coronary Artery Calcification, and Cardiovascular Events," Pursnani et al.) They identified 2435 people from the Framingham study who had never taken statins. Their medical history allowed the authors to determine that, based on the old guidelines, 14% would have been 'statin eligible' compared with 39%, based on the new 2013 guidelines.
Among those eligible by the old guidelines, 6.9% (24/348) developed CVD compared with 2.4% (50/2087) among noneligible participants (HR, 3.1; 95% CI, 1.9-5.0; P less than .001). Under the new guidelines, among those eligible for statins, 6.3% (59/941) developed incident CVD compared with only 1.0% (15/1494) among those not eligible (HR, 6.8; 95% CI, 3.8-11.9; P less than .001).
So, put a whole lot more people on statins, and you prevent an additional very small number of CVD events; 1.0% vs 2.4%. And, 93% of those ‘eligible’ for statins did not develop disease. Nor, of course, do statins prevent all disease. Actually, if everyone in the population were covered, statins would be preventing as many events as they could possibly prevent, but in a small minority of the population. That is, 90+% of people considered to be at 'high-risk' of disease don't go on to develop disease. Is it worth the side effects and cost to put so many more people on statins to prevent the 1.4% more CVD that these new guidelines are preventing? Well, heart disease is still the number one killer in rich countries, and 40+% of the population is currently taking statins, so a lot of people have decided that the benefits do outweigh the risks.
Another question, though, is more fundamental, and it concerns prediction. The calculator seems to now be predicting risk with some confidence. But, let's take a hypothetical person with a somewhat elevated risk. Her cholesterol is higher than the person above who's at lowest risk, but that's due to her HDL. Her systolic blood pressure is high at 180, which is apparently what bumps up her risk, but her 10-year risk is still not over 7.5% so the recommendation is not statins, but lifestyle and nutrition counseling. (Though, the definition of 'heart-healthy diet' keeps changing, so what to counsel this person with low risk seems a bit problematic, but ok.)
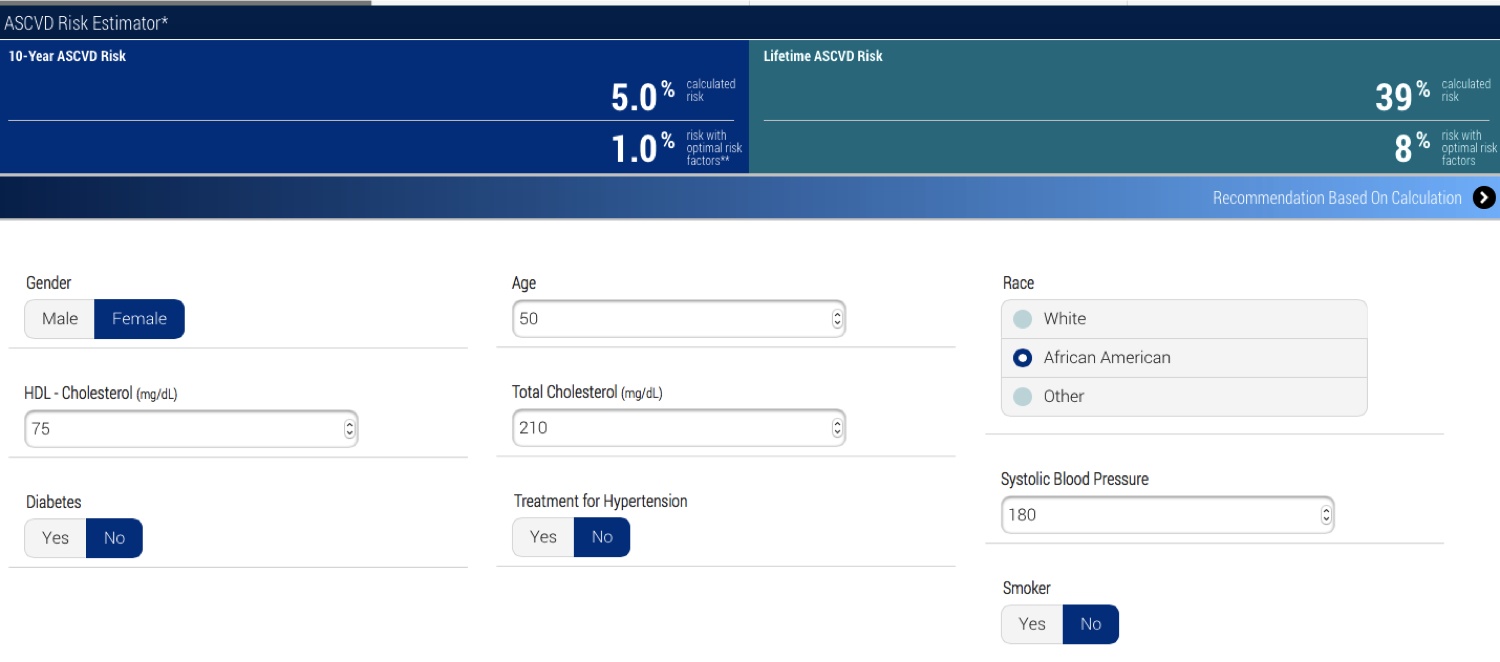 |
| Low enough risk that statins aren't advised. |
Now here's the same hypothetical person, but she's now a smoker, on medication to lower her blood pressure (and her b.p. is still high) and she has diabetes. Her 10-year risk of ASCVD jumps to 36.8%. This makes sense, given what we know about risk factors, right? The recommendation for her is high-intensity statins and lifestyle changes -- lose weight, do regular aerobic exercise, eat a heart-healthy diet, stop smoking (easy enough to say, so hard to do, which is another issue, of course, and the difficulty of changing all these behaviors is one reason that statins are so commonly prescribed).

But now I've lowered her total cholesterol by 70mg/dL, which is what statins ideally would do for her. Even so, the American College of Cardiology/American Heart Association recommendation is for 'high-intensity statin therapy' and lifestyle counseling. The calculator doesn't know this, but statins have already done everything they are likely to do for her.

So, let's add lifestyle changes. But, even when she quits smoking, her 10-year risk is 20%. So let's say we cure her diabetes -- even then, she's still at high enough risk (9%) that 'moderate to high-intensity statins' are recommended. I'm confused. I think even the calculator is confused. It seems there's a fuzzy area where statins are being recommended when what's left to do is, say, lower blood pressure, which statins won't do. This hypothetical woman probably needs to lower her weight to do that, and statins aren't going to help with that, either, but still they're recommended. Indeed, one of the criticisms of this risk calculator when it was released in 2013 was that it overestimates risk. Perhaps so, but it also seems to overestimate the benefit of statins.
Further, it seems there are a lot of type 1 errors here. That is, a lot of people are considered 'at-risk' who wouldn't actually develop cardiovascular disease. Risk of 7.5% means 7.5 of 100 people with a given, equal set of risk factors are expected to develop disease. That means that 92.5 would not. And that means that we have a pretty rough understanding of heart disease risk. The strongest risk factors we know -- smoking, high LDL-C, diabetes and hypertension -- can be expected to predict only a small fraction of events.
And that means that either something else is 'causing' cardiovascular disease in addition to these major known risk factors, or something is protecting people with these risk factors who don't go on to develop disease. Family history is a good or even the very best single predictor (why isn't it taken into account in these calculators?) which suggests that it's possible that genetic risk (or protection) is involved, but genome wide association studies haven't found genes with large effects. Of course, family history is highly conflated with environmental factors, too, so we shouldn't simply assume we need to look for genes when family history indicates risk. Anyway, it's unlikely that there are single genes responsible for ASCVD except in rare families, because that's the nature of complex diseases. Instead, many genes would be involved, but again as with most complex diseases, they would surely be interacting with environmental risk factors, and we don't yet know understand how to identify or really understand gene by environment interaction.
And then there's the truly wild card! All of these risks are based on the combinations of past exposures to measured lifestyle factors, but the mix of those and the rise of other new lifestyle factors, or the demise of past ones, means that the most fundamental of all predictors can itself not be predicted, not even in principle!
So, statins are a very broad brush, and a lot more people are being painted with them than in fact need to be. The problem is determining which people these are, but rather than zoom in with more precision, the updated calculator instead paints a whole lot more people with the brush. This isn't the calculator's fault. It's because understanding risk is difficult, ASCVD is a large and heterogeneous category, and prediction is very imprecise -- even for many 'simple' Mendelian disorders. If ASCVD were caused by a single gene, we'd say it had very low penetrance. And we'd want to understand the factors that affect its penetrance. That's the equivalent to where we are with cardiovascular disease.
I was interested to see that the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk says something that I have said so many times that I decided not to say it again in this post. But, I'm happy to see it elsewhere now. The guideline committee itself acknowledges the issue, so I'll let them explain the problem of assessing risk as their calculator does.
Finally, here's a meta-thought about all this. Ken and I were in Finland this month co-teaching a course, Logical Reasoning in Human Genetics, with colleagues, including Joe Terwilliger. Joe said multiple times, "We suck at finding candidate genes because we don't know anything about biology. We're infants learning to crawl." The same can be said about epidemiological risk factors for many complex diseases -- we suck at understanding the causes of these diseases, and thus we suck at prediction, because we don't really understand the biology.
And that means that either something else is 'causing' cardiovascular disease in addition to these major known risk factors, or something is protecting people with these risk factors who don't go on to develop disease. Family history is a good or even the very best single predictor (why isn't it taken into account in these calculators?) which suggests that it's possible that genetic risk (or protection) is involved, but genome wide association studies haven't found genes with large effects. Of course, family history is highly conflated with environmental factors, too, so we shouldn't simply assume we need to look for genes when family history indicates risk. Anyway, it's unlikely that there are single genes responsible for ASCVD except in rare families, because that's the nature of complex diseases. Instead, many genes would be involved, but again as with most complex diseases, they would surely be interacting with environmental risk factors, and we don't yet know understand how to identify or really understand gene by environment interaction.
And then there's the truly wild card! All of these risks are based on the combinations of past exposures to measured lifestyle factors, but the mix of those and the rise of other new lifestyle factors, or the demise of past ones, means that the most fundamental of all predictors can itself not be predicted, not even in principle!
So, statins are a very broad brush, and a lot more people are being painted with them than in fact need to be. The problem is determining which people these are, but rather than zoom in with more precision, the updated calculator instead paints a whole lot more people with the brush. This isn't the calculator's fault. It's because understanding risk is difficult, ASCVD is a large and heterogeneous category, and prediction is very imprecise -- even for many 'simple' Mendelian disorders. If ASCVD were caused by a single gene, we'd say it had very low penetrance. And we'd want to understand the factors that affect its penetrance. That's the equivalent to where we are with cardiovascular disease.
I was interested to see that the 2013 ACC/AHA Guideline on the Assessment of Cardiovascular Risk says something that I have said so many times that I decided not to say it again in this post. But, I'm happy to see it elsewhere now. The guideline committee itself acknowledges the issue, so I'll let them explain the problem of assessing risk as their calculator does.
By its nature, such an approach requires a platform for reliable quantitative estimation of absolute risk based on data from representative population samples. It is important to note that risk estimation is based on group averages, which are then applied to individual patients in practice. This process is admittedly imperfect; no one has 10% or 20% of a heart attack during a 10-year period. Individuals with the same estimated risk will either have or not have the event of interest, and only those patients who are destined to have an event can have their event prevented by therapy.It's the problem of using group data, which is all we've got, to make clinical decisions about individuals. It's the meta-analysis problem -- meta-analyses compile data from many individual studies to produce a single result that certainly reflects all the studies, because they were all included in the statistics, but it doesn't represent any of them with precision. Ultimately, it's the problem that these sorts of inferences must be based on statistical analysis of samples -- collections -- of individuals. We do not have an easy way around this, including the N of 1 studies currently being proposed.
Finally, here's a meta-thought about all this. Ken and I were in Finland this month co-teaching a course, Logical Reasoning in Human Genetics, with colleagues, including Joe Terwilliger. Joe said multiple times, "We suck at finding candidate genes because we don't know anything about biology. We're infants learning to crawl." The same can be said about epidemiological risk factors for many complex diseases -- we suck at understanding the causes of these diseases, and thus we suck at prediction, because we don't really understand the biology.


Hiç yorum yok:
Yorum Gönder